As I wrote in a previous piece, sometimes what might appear to be a huge medical challenge such as the Coronavirus when analyzed more closely, is really a logistical fight. This will be especially true in the development, manufacture and distribution of test materials and equipment. This is a fight more suited to the private sector than the Center For Disease Control, as has already been most ably demonstrated by our allies, the Republic of (South) Korea.
Which brings us to a point made by my good friend and colleague Nick Arama who notes that once we flood the zone with test kits, the number of confirmed cases of Coronavirus will take a significant jump. However, that might not portend bad news.
Death is the one relatively firm data point we have for the virus since those in bad condition would likely have made it to the hospital. Yet we still have a very low number there, being in the 40s. [now 68 as of this article].
What does that mean? That means that while the number of people who have been diagnosed with it will jump, the deaths haven’t jumped yet. That means that the actual morbidity rate which people have estimated as somewhere between 1-2% based on what we know now, may likely drop below 1%.
First of all, some definitions. For the purposes of this article:
Total Cases-The total persons in the United States who have been infected by Coronavirus (including repatriated citizens/residents).
Total Fatalities—The total persons in the United States who have died from Coronavirus.
Mortality Rate (M/R)—The percentage of persons in the United States who died after contracting Coronavirus.

The left side of the first chart shows a simple table with Date, Infections, Fatality and Mortality Rate. The chart starts with February 29th, as it is the date the first American died on U.S. soil. Note that the Mortality Rate went from 1% to over 7% before declining steadily until it reached just under 2 percent (1.83 as of 2359 GMT, 15- March.
The right side of the chart graphically shows the Mortality Rate and the number of Fatalities. although we will need more data, it appears that the Mortality Rate appears to be leveling off after a rapid decent. However, as my colleague Nick Arama has indicated, this may change as more test kits become available.
This next chart shows how this could work. The table on the left shows the same date range as above. The next column is the Mortality Rate using the number of known infections. Columns 3, 4 and 5 show what the Mortality Rate would be if for each known person infected, there were 1, 2 or 3 others infected but not yet counted.

As my colleague has indicated, as tests become more available, we are very likely to see greatly increased numbers of infected Americans. However, if these trends continue, we could very well see as Arama has said, Mortality rates below 1 percent. I’m not making any scotch wagers just yet, but I am “cautiously optimistic,” and you should be too.
Jerry Giordano
I’m finding myself in a shrinking minority with respect to my view of the WuFlu. To me, it still appears to be an irrational panic. Heather MacDonald still seems to be on my side, at least as of yesterday (article here). But even the Daily Wire guys have been convinced that there is something serious to fear, other than fear itself. By Monday, MacDonald and I may be the only skeptics left standing. (I would find her to be good company in such an event.)
I’ve done a bit of digging into the facts, and I still can’t understand the cause for alarm. I would particularly value the input of our Ricochet docs and other medical professionals, as I certainly realize that I could be wrong.
I. The Severity of the Symptoms
In round numbers, based on the Chinese experience thus far, it appears that about 80% of WuFlu cases are mild, about 15% are “serious,” and about 5% are “critical.” The main problem with the WuFlu seems to be pneumonia. My impression is that “serious” cases might require hospitalization and oxygen treatment, while “critical” cases might require ICU treatment such as intubation. My source is here, from the same Worldometer site that our friend Rodin is relying upon for his daily posts. These estimates are based on information from China through Feb. 11.
Even these figures seem too high to me. Rodin’s daily post today (here) generally shows lower rates of serious/critical cases than the 20% combined figure noted above. In Italy, it is less than 10% (1,518 serious/critical out of 17,750 active). In South Korea, it is less than 1% (59 serious/critical out of 7,300 active). In the US, it is less than 0.5% (10 serious/critical out of 2,395 active).
My suspicion is that the rates of serious or critical illness is much lower, and that the rates appear high because very few people have been tested. This makes sense, as I would expect that initial testing would be limited to people exhibiting WuFlu symptoms. South Korea seems to have done the most extensive testing to date, and its very low rate of serious/critical cases is consistent with the hypothesis that wider testing will show a higher prevalence of the WuFlu, with the vast majority of cases being so mild as to be almost unnoticeable.
II. The Math on the Hospital Bed Crisis
I’ve seen news reports that the WuFlu has overwhelmed the health care system, in Italy in particular. Here is an article from The Atlantic on Wednesday, March 11, stating:
Today, Italy has 10,149 cases of the coronavirus. There are now simply too many patients for each one of them to receive adequate care. Doctors and nurses are unable to tend to everybody. They lack machines to ventilate all those gasping for air.
This NYT article from Thursday, March 12 similarly claims, in its headline:
We don’t have enough ventilators and I.C.U. beds if there’s a significant surge of new cases. As with Italy, the health system could become overwhelmed.
I know that I’m just a country lawyer, though I did once study math through the graduate level, with a focus on probability, statistics, and mathematical modeling. But it doesn’t take grad-level math to question these figures. It takes middle-school algebra.
The NYT article linked above says that Italy has 3.2 hospital beds per 1,000 people (and the US has only 2.8 beds per 1,000 people). Italy has a population of about 60 million, so this implies about 192,000 hospital beds.
As noted above, the number of serious or critical WuFlu cases reported in Italy, according to Rodin’s post today, is 1,518. That is 0.79% of the number of hospital beds in Italy.
Think about that. We’re supposed to believe that an influx of about 1,500 new patients has overwhelmed the medical system of a nation that has 192,000 hospital beds.
Put this in perspective. Let’s round up the Italian number to 1% — that is, assume that the number of serious or critical WuFlu cases in Italy is equal to 1% of the country’s hospital beds. Imagine that you run a hospital with 200 beds. This means that you can expect two (2) extra patients as a result of WuFlu. Are people seriously suggesting that a 200-bed hospital will be “overwhelmed” if it has to take in an additional two patients?
How many serious or critical cases are there in the US? Ten (10), according to Rodin’s post today. But let’s assume that the WuFlu spread rapidly in the US over the next month. How rapidly? Well, China has had 80,000 cases over several months, so let’s make the extreme assumption that the US has 100,000 new cases over the next month — a vastly faster spread than in China. And let’s use the Chinese figures for serious and critical cases, rather than the much lower figures from South Korea (more than 20 times lower).
So if the US has 100,000 new cases over the next month, 15% will be serious (15,000) and 5% will be critical (5,000), for a total of 20,000. This would be about 13 times the number of serious or critical cases currently existing in Italy.
20,000 new cases in the US would represent about 2.2% of the hospital beds in the country. A hypothetical hospital with 200 beds would have to take in about 4 new patients over the next month.
Is the medical profession seriously maintaining that their capabilities are so marginal, their ability to adapt so limited, as to be unable to cope with an increase in their patient load of about 2%?
I fully understand the graph about the capacity of the health system. Here is one example:
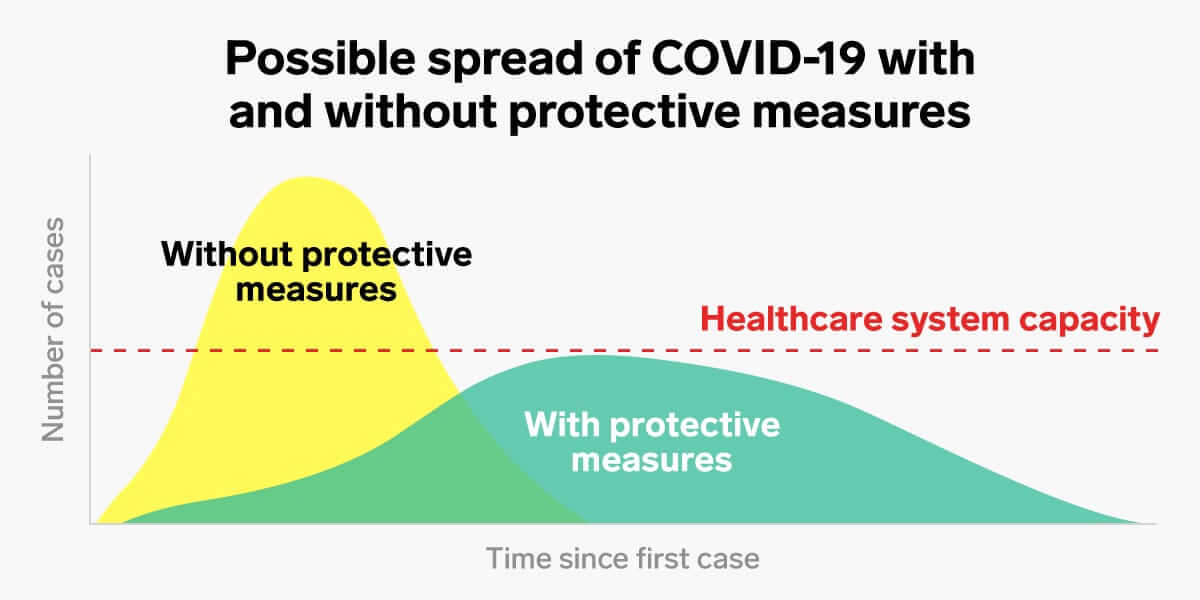
I do not dispute this graph in theory. I dispute the dashed red line about the “healthcare system capacity.” Based on my calculations above, the dashed red line is nowhere near as low as indicated. It is far, far higher — literally off the chart, in this graph.
As noted above, I don’t just understand mathematical modeling. I am a lawyer. I know how to mislead — in my case, I endeavor not to mislead myself, but I am ever vigilant about how my opposition can mislead. This is precisely the way that one can generate a panic — with a graph that is correct in theory, with just one small misleading element.
I see no evidence whatsoever of any serious danger that the WuFlu will overwhelm our healthcare system capacity, even with no protective measures.
Another way to mislead, incidentally, is to assume that the number of cases will continue to grow exponentially. The very early stages seem exponential, but the number of cases eventually follows an S-curve. Continuing to project an exponential growth rate — say for an entire month — is contrary to the facts, and will lead to a vast overestimate of the number of cases that we can expect.
IV. About That March Madness
Actually, perhaps these hypothetical WuFlu patients will be able to watch March Madness. Because, it seems to me, the term is being redefined.
I was expecting to watch March Madness on CBS Sports and ESPN. It was going to involve a bunch of college basketball players. Now, I seem to be watching a different kind of March Madness on CNN, MSNBC, and Fox News. It involves a bunch of talking heads, politicians, and medical experts telling me that we’re all going to die unless we shut down the world. I find this extremely unlikely.
I would appreciate any corrections to my analysis.
If I turn out to be correct, I am going to prepare a huge plate of crow for everyone who disagreed. :)
As Shutdown Mania picked up the pace the past few days it was disturbing to watch how readily people were willing to toss away some rights in the name of public health. Social media broke into two camps: those who are taking anything our government overlords are telling us, and those -- like me -- who are skeptical that all of this is necessary.
Gov. Gavin Newsom closed all of California’s bars right before St. Patrick’s Day, and also basically grounded Golden State residents over the age of sixty-five.
That’s a lot of people out of work for one of the biggest bar business days of the year.
What worries me is that a lot of politicians are in “never let a crisis go to waste” mode now and are using the panic to become heavy-handed nanny state types, perversely using this as their moment to shine.
An old friend of mine from Los Angeles put it rather succinctly:
People are going to be out of work and money, and the pandering politicians have rushed in to assure them that the government will “help.” We’re tanking the economy but the government is going to magically have money to give to its citizens. Nobody has been able to successfully walk me through the math on that one yet.
This is going to be a brief Briefing today because there are only so many ways I can write “PUMP THE BRAKES!” I’m out of quarantine now but there is no place to go because everything but the grocery stores are closed. I’m waiting for the government to shut down domestic air travel soon, so we can all go full Hunger Games on each other.
No comments:
Post a Comment